Göztepe Education and Research Hospital, Pediatric Endocrinology Clinic, İstanbul, Türkiye
OBJECTIVE: Congenital adrenal
hyperplasia (CAH) can be complicated by central precocious puberty (CPP) in
children, which may compromise final height. We aimed to evaluate the effect of
gonadotropin-releasing hormone analog (GnRHa) therapy on growth in children
with CAH.
DESIGN: Twelve children with CAH were enrolled in a follow-up study.
Eight patients underwent the GnRH stimulation test. GnRHa-treatment was
administered at 3.75 mg every 4 weeks; the dose had to be increased to 7.5 mg
in three patients. Bone age, growth velocities and body mass index of the
patients were monitored during treatment.
RESULTS: Median chronologic age and
bone age at diagnosis were 6.8 (3.5) years and 11 (1.2) years, respectively.
Median follow-up was 4.4 (4.9) years. A significant difference was found in the
median ratio of bone age to chronological age between diagnosis and last visit
(p=0.005) and between the beginning of GnRHa treatment and last visit
(p=0.004). Median growth velocity was 4 (2.5) cm, 3.4 (5.2) cm and 5.5 (5.5) cm
at the end of the first, second and third years of the therapy, respectively.
Second-year growth velocity was inversely correlated with median bone age at
diagnosis (rho:-0.758, p=0.004) and at the initiation of therapy (rho:-0.876,
p<0.001).
CONCLUSION: GnRHa therapy should be considered for augmentation of
linear growth and diminishment of bone age advancement in children with CAH
complicated by CPP, particularly in children who do not have extremely advanced
bone age for chronological age.
Childhood, Congenital adrenal hyperplasia, Leuprolide acetate, Precocious puberty
INTRODUCTION
In patients with congenital adrenal hyperplasia (CAH), final height may be compromised due to high levels of androgens.1 A compromised final height is more prominent in patients unsuitable for treatment and in undertreated and overtreated patients.2 Indeed, elevated adrenal androgen production causes an alteration in bone age with loss of growth potential.3 Chronic mildly to moderately elevated androgens or intermittent hyperandrogenemia may trigger the activation of the hypothalamic-pituitary axis (HPA) leading to central precocious puberty (CPP) which is frequently seen in these patients.4-6 In a number of countries, the diagnosis of CAH can be established early through neonatal screening programs. However, in countries where no routine screening for CAH is implemented, the diagnosis is delayed and patients usually present later with clinical findings of hyperandrogenemia. Gonadotropin releasing hormone analogs (GnRHa) have been used effectively in the treatment of CPP for many years. By consistent stimulation of gonadotrophic hormones, GnRHa bring about inhibition of cyclic secretion of these hormones and prevent the progression of puberty.7 Our aim in this study was to investigate the effect of GnRHa treatment on growth in patients with CAH complicated by CPP.
MATERIAL AND METHODS
Patients
Age at diagnosis is defined as the age of the patient when first admitted to our clinic. Twelve patients aged 2.4-8.8 years who had been monitored at a pediatric endocrinology clinic with the diagnosis of CAH and signs of CPP were enrolled in this observational study. Ten patients had the simple virilizing CAH form, while two had the salt-wasting form. On first admission, detailed clinical histories of the patients were obtained and anthropometric measurements were taken with light clothing using a digital scale and a Harpenden stadiometer. The body mass index (BMI) was calculated as the ratio of weight/height2 (kg/m2). BMI and height were expressed as standard deviation score (SDS) using the Turkish reference data.8 All physical examinations were performed by the same physician (AG) and the findings were recorded. Pubertal stage was assessed by physical examination according to Tanner staging for breast development in females and for volume of both testes in males.9,10 Precocious puberty was defined as testicular growth before the age of nine in boys and increased breast growth before the age of eight in girls. Stretched penil length and testicular volume determined by using Prader orchiometry in boys and breast stage in girls were recorded during examination. A single observer (AG) performed a bone age assessment using the Greulich and Pyle method.11 Bone age advancement was defined as the difference between bone age and chronological age expressed in years. Target height (TH) was calculated at diagnosis (TH was calculated using the formula: [maternal height + paternal height – 13 cm for girls and + 13 cm for boys]/2). Predicted adult height (PAH) was calculated at diagnosis and at last visit using the Bayley and Pinneau (B&P) method Bonfig and Schwarz (B&S) approach.12,13 Respective B&P tables were used for patients with average bone age (within one year of chronological age), retarded bone age (delayed by more than one year) and accelerated bone age (accelerated by more than one year). PAH-SDS was also calculated in both methods. Ratio of bone age to chronologic age was assessed at diagnosis, at initiation of GnRHa therapy (GnRHa-T) and at last visit.
Endocrine work-up
Morning blood samples obtained from eight CAH children for basal androgens and precursor levels [delta-1-4-androstenedione, dehydroepiandrosterone sulfate (DHEAS), testosterone and 17-hydroxyprogesterone (17OHP)] and the adrenocorticotropic hormone stimulation test (ACTH, Synacthen, 250 µg intravenously) was performed in all children except in two boys diagnosed with salt-wasting CAH in infancy (patients 6 and 7). A GnRH stimulating test was performed in all patients except the four with basal serum gonadotropin levels consistent with CPP (patients 1, 5, 8 and 11). After blood basal gonadotropin levels were tested, luteinizing hormone-releasing hormone (Ferring ampul, 100µgr) was administered intravenously and 30-, 60- and 90-minute blood samples were tested for luteinizing hormone (LH) and follicle-stimulating hormone (FSH). Stimulated LH levels if over 5mIU/mL (immunochemiluminometric assay) were considered pubertal.14 We also considered as CPP associated with LH/FSH a peak ratio more than 0.3. In addition to LH and FSH, E2, total testosterone, DHEAS, cortisol and ACTH were measured with immunoenzymatic methods (Beckman Coulter, DXI 800, USA). An Immunotech assay kit (Beckman Coulter) and the radioimmunoassay method (ICN ISO DATA Gamma Counter) were used to measure17-hydroxyprogesteron and 1,4-androstenedion levels.
Imaging studies
Pelvic ultrasonography was performed in patients with 46,XX karyotype and surrenal ultrasonographic examination was performed in all patients. Ovarian volume was calculated with the formula [(length X width (mm) × height (mm) × 0.523/1000 (ml)].15 Pituitary and cranial magnetic resonance imaging (MRI) was performed in eight patients with CPP.
Mutation analysis
All patients underwent confirming mutational analysis of the CYP21A2 gene.
Therapy and follow-up
All patients were treated with hydrocortisone. Mineralocorticoid treatment was added in two patients. Treatment was expected to be lifelong in all cases. Indications of the treatment with GnRHa were as follows: Observation of clinical signs of puberty (Tanner stage 2) before the chronological age of eight in girls and before the chronological age of nine in boys, confirmation of precocious puberty with elevated basal and/or stimulated LH and FSH levels and advancement of bone age for chronological age. GnRHa therapy (Leuprolide acetate) was administered at 3.75 mg every 4 weeks; the dose had to be increased to 7.5 mg in three children (cases 5, 8, 10) who had a higher LH response to GnRHa of more than 2.5 IU, 90 minutes after injections.16 Therapy was stopped in eight patients (nos. 1, 3, 5, 6, 8, 9, 10 and 11) due to advanced bone age during the last visit. All patients with CAH complicated by CPP were examined at 3-month intervals. Bone ages, growth velocities and body mass indexes (BMI) of patients during treatment were evaluated.
Statistical analysis
All statistical analyses were performed by using the SPSS 18.0 (SPSS for windows, SPSS Inc, Chicago, Illinois, USA) statistical package program. Descriptive statistics were presented as median values with interquartile ranges. The paired Wilcoxon test was used for comparisons. Spearman’s correlation method was used in correlation analysis and the correlation coefficient was accepted as rho. Significance was evaluated at p <0.05.
RESULTS
The study population was comprised of twelve patients with CAH. The features of the patients at diagnosis, at the beginning of GnRHa therapy and at the last visit are presented in Table 1. Five children have 46,XX karyotype; one of them was raised as a male.
The follow-up duration was 4.4 (4.96) years. Median time between admission and beginning of GnRHa therapy was 0.8 (0.56) years (Table 1); this time was less than six months in four patients (patients 3, 5, 8 and 11).
The results of the genetic analysis are presented in Table 2. All boys including the one with 46,XX karyotype had increased penile length. Four girls had clitoromegaly and one girl had clitoroplasty (patient 3). Physical examination and ultrasonographic findings are presented in Table 2. Median basal and stimulated LH levels were 1 (0.4) uIU/mL and 16.3 (12.4) uIU/mL, respectively. The detailed hormonal investigations are presented in Table 3.
All children underwent GnRHa treatment. Treatment was maintained for over three years in seven patients, for 2.5-3 years in two patients and for less than two years in three patients. Median duration of therapy was 3.8 (2.1) years. Predicted adult height was calculated at diagnosis as 149.2 (27.4) cm (n:10) according to the B&P method and as 146.6 (22.3) cm (n:8) according to the B&S method. Predicted adult height at last visit was 154 (13) cm according to the B&P method and 154.5 (22.3) cm according to the B&S method. The B&P method was not used to calculate PAH at diagnosis as bone age was less than six in patients 7 and 12, while the B&S method was not used to calculate PAH at diagnosis in patients 1, 7, 9 and 12 (Table 2). There was no difference between PAH and PAH-SDS as per the B&P method on diagnosis and in last visit (p=0.721). However, a significant difference was found in PAH (p=0.012) and PAH-SDS (p=0.012) according to the B&S method between diagnosis and last visit. A significant difference was found between median ratio of bone age/chronological age ratio at diagnosis and at last visit (p=0.004), and at diagnosis and the beginning of therapy (p=0.005) (Figure 1). There was no difference in testicular volume of the boys and breast size of the girls between diagnosis and the last visit (p=0.084, p=0.182, respectively). Median growth velocity was, respectively, 4 (2.5) cm, 3.4 (5.2) cm and 5.5 (5.5) cm at the end of the first, second and third years of the therapy (n:8). First-year growth velocity did not differ from second-year growth velocity (p=0.784) and third-year growth velocity (p=0.058). Median second-year growth velocity was inversely correlated with bone age at diagnosis (rho: -0.758; p=0.004) and bone age at the beginning of GnRHa therapy (rho: -0.876, p<0.001). Median third-year growth velocity was inversely correlated with bone age at diagnosis (rho: -0.826; p=0.011).
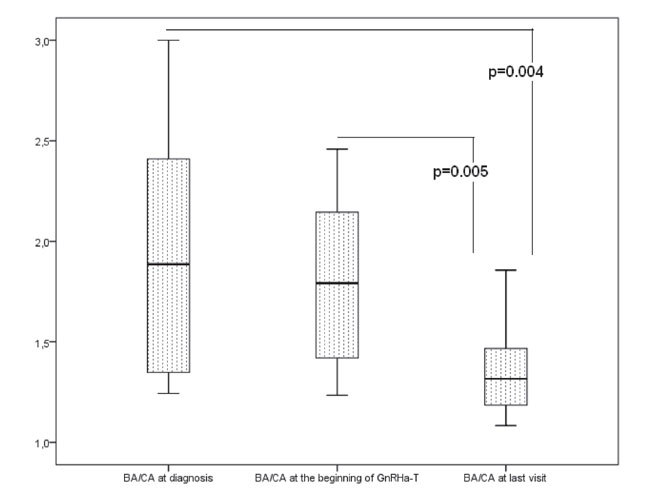
Figure 1. Ratios of bone age to chronological age (BA/CA) at diagnosis, at the beginning of GnRH analog therapy and at last visit.
DISCUSSION
Twelve patients with CAH complicated by CPP were evaluated. Since there is no neonatal screening program for CAH in our country, the diagnosis of almost all patients was late in our study population. All patients were diagnosed with CAH on their first admission and were treated as soon as possible. Moreover, almost all patients had clinical findings of hyperandrogenemia, with some of them having CPP on first admission. Of these, three had increased basal and stimulated gonadotropin levels consistent with CPP and were immediately started on GnRHa treatment.
We found that bone age at initiation of GnRHa therapy was the most important factor affecting the growth velocity and that height of the patients at diagnosis was inversely correlated with the ratio of bone age to chronological age at last visit. These results indicated that the CAH patients with advanced bone age at the time of diagnosis had decreased growth velocity, which was consistent with a previous research project.5 Another important finding was the decreased bone age/chronological age ratio in patients after treatment, which suggests that GnRHa treatment slows down bone age advancement in patients with CAH complicated by CPP, which could help improve linear growth. GnRHa treatment of CAH and CPP was first described in 1985 by Pescovitz et al.4 In this study, four patients with CAH caused by 21-hydroxylase deficiency were treated with GnRHa in addition to hydrocortisone and fludrocortisone. This regimen provided a regression of testicular enlargement in boys and breast development in girls. Furthermore, GnRH stimulating tests during treatment demonstrated suppression of LH and FSH levels. The treatment also slowed down growth velocity and bone age advancement. Dacou-Voutetakis et al5 investigated eight CAH patients who started glucocorticoid treatment at advanced ages. All eight of them had CPP; four were treated with luteinizing hormone-releasing hormone agonist and four were monitored as control subjects. While there was no difference between target height and final height in the treatment group, the final height in the control group fell behind the target height. In their study of six patients with CAH complicated by CPP, Soliman et al6 suggested that GnRHa should be added to hydrocortisone and fludrocortisone treatment and should be maintained for at least two years. Although they observed a decrease in growth velocity in the first two years of therapy, PAH improved and bone advancement slowed down. The calculation of PAH is essential in these patients when planning treatment for augmentation of linear growth. In their recently published study, Bonfig and Schwarz13 revealed that the predicted height was overestimated in patients with CAH. We used their approach in addition to the B&P method and, while there was improvement in PAH with treatment, it was statistically insignificant according to the B&P method. On the other hand, there was a difference between PAH at diagnosis and at last visit according to the B&S method. The latter method needs further research and larger patient samples. In consistence with other studies, a statistically insignificant improvement of linear growth was observed in CAH patients after GnRHa treatment.4,6 Growth hormone (GH) treatment in addition to GnRHa has been rated among the therapies improving linear growth in patients with precocious puberty.17 According to Lin-Su et al,18,19 supplementing GnRHa treatment with GH was beneficial for final height in patients with CAH. We did not use GH therapy in our patients as it is only recommended for patients with low growth velocity and GH deficiency in our country.
CONCLUSION
The present study demonstrated that CPP can be observed at the time of diagnosis in patients belatedly diagnosed with or undertreated for CAH. Central precocious puberty can be a complication of CAH, particularly in countries where a routine neonatal screening program for this condition is lacking. Bone age at diagnosis and at the beginning of GnRHa treatment was the most important factor for growth velocity in the patients with CAH complicated by CPP. Moreover, GnRHa treatment alone was able to slow down bone age advancement, resulting in a slight improvement in PAH. As patients with advanced bone age have diminished growth velocity, we suggest that treatment be started immediately in the presence of clinical or laboratory findings consistent with CPP.
FUNDING
This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector.
CONFLICT OF INTEREST
None of the authors has personal or financial conflicts of interest.
REFERENCES
1. White PC, Speiser PW, 2000 Congenital adrenal hyperplasia due to 21-hydroxylase deficiency. Endocr Rev 21: 245-291.
2. Lim YJ, Batch JA, Warne GL, 1995 Adrenal 21-hydroxylase deficiency in childhood: 25 years’ experience. J Paediatr Child Health 31: 222-227.
3. Jääskeläinen J, Voutilainen R, 1997 Growth of patients with 21-hydroxylase deficiency: an analysis of the factors influencing adult height. Pediatr Res 41: 30-33.
4. Pescovitz OH, Cassorla F, Comite F, Loriaux DL, Cutler GB Jr, 1985 LHRH analog treatment of central precocious puberty complicating congenital adrenal hyperplasia. Ann N Y Acad Sci 458: 174-181.
5. Dacou-Voutetakis C, Karidis N, 1993 Congenital adrenal hyperplasia complicated by central precocious puberty: treatment with LHRH-agonist analogue. Ann N Y Acad Sci 687: 250-254.
6. Soliman AT, Al Lamki M, Al Salmi I, Asfour M, 1997 Congenital adrenal hyperplasia complicated by central precocious puberty: linear growth during infancy and treatment with gonadotropin-releasing hormone analog. Metabolism 46: 513-517.
7. Partsch CJ, Heger S, Sippell WG, 2002 Management and outcome of central precocious puberty. Clin Endocrin 56: 129-148.
8. Neyzi O, Furman A, Bundak R, Gunoz H, Darendeliler F, Bas F, 2006 Growth references for Turkish children aged 6 to 18 years. Acta Paediatr 95: 1635-1641.
9. Marshall WA, Tanner JM, 1969 Variations in pattern of pubertal changes in girls. Arch Dis Child 44: 291-303.
10. Marshall WA, Tanner JM, 1970 Variations in the pattern of pubertal changes in boys. Arch Dis Child 45: 13-23.
11. Greulich WW, Pyle SI 1959 Radiographic atlas of skeletal development of the hand and wrist. Stanford University Press, Palo Alto.
12. Bayley N, Pinneau S, 1952 Tables for predicting adult height from skeletal age: revised for use with Greulich-Pyle hand standards. J Pediatr 40: 423-441.
13. Bonfig W, Schwarz HP, 2012 Overestimation of final height prediction in patients with classical congenital adrenal hyperplasia using the Bayley and Pinneau method. J Pediatr Endocrinol Met 25: 645-649.
14. Carel JC, Lahlou N, Roger M, Chaussain JL, 2004 Precocious puberty and statural growth. Hum Reprod Update 10: 135-147.
15. Badouraki M, Christoforidis A, Economou I, Dimitriadis AS, Katzos G, 2008 Evaluation of pelvic ultrasonography in the diagnosis and differentiation of various forms of sexual precocity in girls. Ultrasound Obstet Gynecol 32: 819-827.
16. Demirbilek H, Alikasifoglu A, Gonc NE, Ozon A, Kandemir N, 2012 Assessment of gonadotrophin suppression in girls treated with GnRH analogue for central precocious puberty; validity of single luteinizing hormone measurement after leuprolide acetate injection.Clin Endocrinol (Oxf) 76: 126-130.
17. Pucarelli I, Segni M, Ortore M, Arcadi E, Pasquino AM, 2003 Effects of combined gonadotropin-releasing hormone agonist and growth hormone therapy on adult height in precocious puberty: a further contribution. J Pediatr Endocrinol Metab 16: 1005-1010.
18. Lin-Su K, Vogiatzi MG, Marshall I, et al, 2005 Treatment with growth hormone and luteinizing hormone releasing hormone analog improves final adult height in children with congenital adrenal hyperplasia. J Clin Endocrinol Metab 90: 3318-3325.
19. Lin-Su K, Harbison MD, Lekarev O, New MI, 2001 Final adult height in children with congenital adrenal hyperplasia treated with growth hormone. Clin Endocrinol Metab 96: 1710-1717.
Corresponding author:
Prof.
Dr. Ayla Güven, Göztepe Eğitim ve Araştırma Hastanesi, Çocuk Endokrin Kliniği,
Dr. Erkin Caddesi, Kadıköy, İstanbul, Türkiye,
Tel.: +90 532 238 03 00, Fax: +90 216 566 4023
Received 27-05-2014, Accepted
18-09-2014